

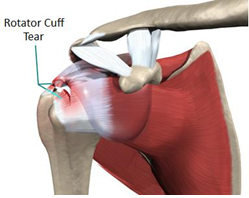
You have a tear of the rotator cuff tendon/s of the shoulder. This has been diagnosed with an arthrogram, an MRI, or ultrasound. The tendons are very important for active movements of the shoulder, particularly elevation. Once the tendon is torn, it will not heal and the tear may progress and increase in size with time. This will result in gradual loss of active motion and an increase in the amount of pain. Typically patients get severe pain with elevation of the arm and discomfort at night. The shoulder will feel weak and tire quickly particularly with overhead use of the arm.
This is a common condition in persons over 5O years of age and can be related to a lifting injury, over-use activities and/or age related degeneration of the muscles and tendons.
 |
 |
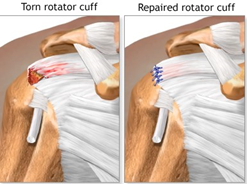
You have elected to undergo a ROTATOR CUFF REPAIR which is a fairly large operative procedure, but usually achieves excellent results.
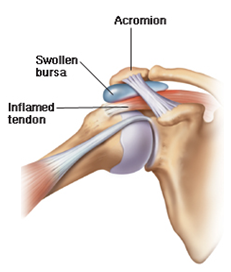
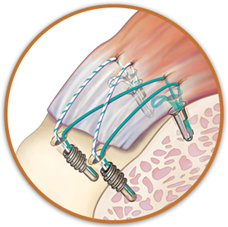
The operation is a key hole procedure and requires making small holes around the shoulder to gain access to the joint using small, delicate instruments. The shoulder joint is examined to fully assess and confirm the diagnosis. Trimming of bone called the ACROMION and excision of a ligament called the CORACO-ACROMIAL ligament helps to enlarge the space in which the rotator cuff tendons lie. The inflamed bursa is also removed. If there is associated arthritis of the acromioclavicular joint then a small portion of bone is removed from the outer end of the clavicle. The rotator cuff is then inspected, contractures released and the tear repaired. Various methods are used but on most occasions, special anchors with sutures are placed into the bone to provide a stable platform to reattach the tendon. The operation usually takes about one and a half hours.
You will wake up in the recovery ward with a sling and binder. Occasionally, the tear is very large and the repair needs to be protected in a sling with bolster to keep the arm away from the side. Massive tears may not be repairable and whilst one can expect improvement in pain, active movement and function may not be regained.
You will be seen by the surgeon the next day and simple passive motion exercises (where the other arm is used to move the shoulder) is commenced to avoid stress to the repair. It is normal to feel some discomfort with the exercises but this can be controlled with regular pain medication. The dressing will be changed and you will be permitted to go home.
The cuff takes up to 3 months to heal to bone and the repair must be protected during this period whilst movement is regained. Exercises should be carried out 3-4 times per day at home. Formal physiotherapy is not required for the first 6 weeks after surgery. A detailed rehabilitation protocol will be given to you before discharge from hospital. In the first 6 weeks you are allowed to shower with your arm by your side. Again, it must be emphasised that under no circumstances are you to elevate the affected arm under its own power.
Follow up in the rooms occurs at 2 weeks when the dressing is taken down and wound inspected. Further instructions will be given in relation to your rehabilitation programme. Active movements do not commence until 6 weeks after surgery and this period may be even longer if the tear is large. Strengthening and resistance exercises commence around 3 months.(For further information on the postoperative rehabilitation protocol, see separately “Rotator Cuff Repair Postop Protocol”.
Physiotherapy can take up to 6 months to achieve a near full range of motion and 12 months to achieve a full range of motion. It is not uncommon for complete pain relief to require at least 12 months of rehabilitation following surgery. Patients should not to return to jobs that involve heavy lifting and overhead activity. This is because there is intrinsic weakness in the tendon and with heavy activity there is always a risk of re-rupture.
The success rate of this surgery is in the vicinity of 90 percent. Even with surgery you will never again have a perfect shoulder but you will have an excellent shoulder and certainly a much better shoulder than prior to surgery.
There are a number of complications that can occur with surgery and these will be discussed with you by your surgeon. In addition to the risks of surgery in general, such as blood loss or problems related to anaesthesia, complications of rotator cuff surgery may include:
Nerve injury. This typically involves the nerve that activates your shoulder muscle (deltoid).
Infection. Patients are given antibiotics during the procedure to lessen the risk for infection. If an infection develops, an additional surgery or prolonged antibiotic treatment may be needed.
Stiffness. Early rehabilitation lessens the likelihood of permanent stiffness or loss of motion. Most of the time, stiffness will improve with more aggressive therapy and exercise.
Tendon re-tear. There is a chance for re-tear following all types of repairs. The larger the tear, the higher the risk of re-tear. Patients who re-tear their tendons usually do not have greater pain or decreased shoulder function. Repeat surgery is needed only if there is severe pain or loss of function.
If after reading this you have any questions be sure to discuss them with your surgeon prior to your operation.
The operation is a key hole procedure and requires making small holes around the shoulder to gain access to the joint using small, delicate instruments. The shoulder joint is examined to fully assess and confirm the diagnosis. Trimming of bone called the ACROMION and excision of a ligament called the CORACO-ACROMIAL ligament helps to enlarge the space in which the rotator cuff tendons lie. The inflamed bursa is also removed. If there is associated arthritis of the acromioclavicular joint then a small portion of bone is removed from the outer end of the clavicle. The rotator cuff is then inspected, contractures released and the tear repaired. Various methods are used but on most occasions, special anchors with sutures are placed into the bone to provide a stable platform to reattach the tendon. The operation usually takes about one and a half hours.
 |
 |
You will be seen by the surgeon the next day and simple passive motion exercises (where the other arm is used to move the shoulder) is commenced to avoid stress to the repair. It is normal to feel some discomfort with the exercises but this can be controlled with regular pain medication. The dressing will be changed and you will be permitted to go home.
The cuff takes up to 3 months to heal to bone and the repair must be protected during this period whilst movement is regained. Exercises should be carried out 3-4 times per day at home. Formal physiotherapy is not required for the first 6 weeks after surgery. A detailed rehabilitation protocol will be given to you before discharge from hospital. In the first 6 weeks you are allowed to shower with your arm by your side. Again, it must be emphasised that under no circumstances are you to elevate the affected arm under its own power.
Follow up in the rooms occurs at 2 weeks when the dressing is taken down and wound inspected. Further instructions will be given in relation to your rehabilitation programme. Active movements do not commence until 6 weeks after surgery and this period may be even longer if the tear is large. Strengthening and resistance exercises commence around 3 months.(For further information on the postoperative rehabilitation protocol, see separately “Rotator Cuff Repair Postop Protocol”.
Physiotherapy can take up to 6 months to achieve a near full range of motion and 12 months to achieve a full range of motion. It is not uncommon for complete pain relief to require at least 12 months of rehabilitation following surgery. Patients should not to return to jobs that involve heavy lifting and overhead activity. This is because there is intrinsic weakness in the tendon and with heavy activity there is always a risk of re-rupture.
The success rate of this surgery is in the vicinity of 90 percent. Even with surgery you will never again have a perfect shoulder but you will have an excellent shoulder and certainly a much better shoulder than prior to surgery.
There are a number of complications that can occur with surgery and these will be discussed with you by your surgeon. In addition to the risks of surgery in general, such as blood loss or problems related to anaesthesia, complications of rotator cuff surgery may include:
Nerve injury. This typically involves the nerve that activates your shoulder muscle (deltoid).
Infection. Patients are given antibiotics during the procedure to lessen the risk for infection. If an infection develops, an additional surgery or prolonged antibiotic treatment may be needed.
Stiffness. Early rehabilitation lessens the likelihood of permanent stiffness or loss of motion. Most of the time, stiffness will improve with more aggressive therapy and exercise.
Tendon re-tear. There is a chance for re-tear following all types of repairs. The larger the tear, the higher the risk of re-tear. Patients who re-tear their tendons usually do not have greater pain or decreased shoulder function. Repeat surgery is needed only if there is severe pain or loss of function.
If after reading this you have any questions be sure to discuss them with your surgeon prior to your operation.
 Dr. Leonard kuo
Dr. Leonard kuo