

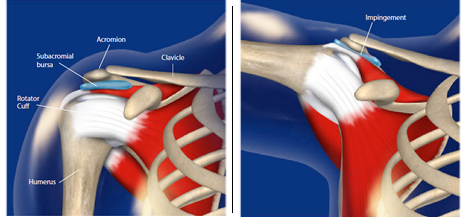
When the rotator cuff tendons become inflamed or partially torn, it may swell and lead to impingement between the head of the humerus and the acromion when the arm is elevated, causing pain. This bone projects over the top of the shoulder and forms part of the shoulder blade bone. It is easily felt as the point of the shoulder.
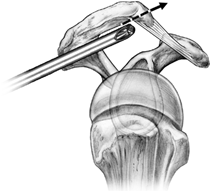
When the inflammation and impingement symptoms do not settle with rest, injections, physiotherapy exercises and rest, more room needs to be created to allow the rotator cuff tendons to move freely. This consists of removal of inflamed tissue that lies over the cuff (bursectomy) and trimming of part of the acromion which may have an associated spur (acromioplasty) and its ligament (coracoacromial ligament).
The operation can be performed arthroscopically. It is minimally invasive surgery performed through small (key hole) incisions and enables the surgeon to look into the shoulder joint, make an exact diagnosis, and treat the impingement. Small and delicate instruments that fit through the small skin incisions are able to visualise the shoulder using a camera. Because this technique disturbs the shoulder joint less than open surgery, the hospital stay is shorter and the recovery smoother. On occasions, we may find something unexpected and the benefit of arthroscopy is that we can fix these problems as well.
On occasions another tendon in the shoulder, called the biceps tendon, is severely damaged and it may be necessary to release that tendon. This procedure does not lead to any functional deficit but may leave a small cosmetic lump in the lower arm. On occasions the tendon is removed from the joint and re attached using a screw to the upper part of the humerus bone.
You will wake up in the recovery ward with a sling and binder. You will be seen by the surgeon the next day and motion exercises are commenced under physiotherapy supervision. It is normal to feel some discomfort with the exercises but this can be controlled with regular pain medication. The dressing will be changed and you will be permitted to go home.
The sling may be worn for several weeks but the arm is taken out for exercise 3-4 times per day. Early motion helps to prevent stiffness and hasten recovery. Even if the shoulder does get stiff in the early post operative period it usually does recover but may take a period of months rather than weeks to do so.
The operation has a six month rehabilitation period and if the Rotator Cuff muscles are not too badly damaged the success rate of surgery is about 90 per cent. The shoulder will continue to improve for up to 12 months. The surgery works by removing the bone that rubs on the Rotator Cuff muscle and relies on the ability of the muscle to heal. We cannot give you a new Rotator Cuff. Unfortunately in about 10 percent of patients, the muscle does not heal and the surgery does not work.
 Dr. Leonard kuo
Dr. Leonard kuo