

PERTHES DISEASE
WHAT IS PERTHES DISEASE?
This childhood condition is caused by disturbance of blood supply to the ball of the hip joint ( femoral head ). We do not know what triggers the condition. The femoral head, like all living tissue requires nutrition which it receives from blood flow through fine blood vessels. In Perthes' disease, a variable number of these vessels are blocked with the result that parts of the femoral head become non-viable (avascular necrosis).
Fortunately the child's hip has great capacity to repair the damage. New blood supply will develop and repair of the damaged bone is usually complete in 2 to 3 years. This happens even if no treatment is given. The rate of repair is inversely proportional to the age of the child, therefore younger children get over the condition quicker and have a better outcome.
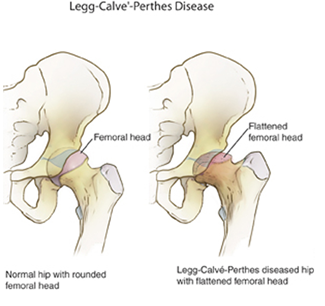
The portion of the femoral head affected by the avascular necrosis is mechanically weak and during the time it takes nature to heal the affected part, deformity may develop. The femoral head is normally spherical and fits perfectly within a cup ( acetabulum ) on the side of the pelvis to form the hip joint. This condition can cause the femoral head to flatten ( non-spherical head ) and grow beyond the confines of the acetabulum (extrusion or subluxation).
The degree of deformity of the femoral head determines the outcome of the condition. Minor deformity is compatible with normal hip function but major deformity may result in premature arthritis of the hip joint.
The portion of the femoral head affected by the avascular necrosis is mechanically weak and during the time it takes nature to heal the affected part, deformity may develop. The femoral head is normally spherical and fits perfectly within a cup ( acetabulum ) on the side of the pelvis to form the hip joint. This condition can cause the femoral head to flatten ( non-spherical head ) and grow beyond the confines of the acetabulum (extrusion or subluxation).
The degree of deformity of the femoral head determines the outcome of the condition. Minor deformity is compatible with normal hip function but major deformity may result in premature arthritis of the hip joint.
PRESENTATION
The condition affects children between the ages of 4 to 10 years though older and younger children can be affected. It usually affects one hip but in 10% of cases both hips are affected. The child with the condition develops a limp which worsens gradually. There is usually pain in the knee, thigh or groin when the child attempts to put weight on the leg or move the hip joint.
The,condition affects only the hip joint and there is no associated general illness. Pain and limp is intermittent initially and becomes gradually more persistent. Mobility of the hip joint is reduced if there is already some deformity of the femoral head, the affected leg is slightly shortened.
The,condition affects only the hip joint and there is no associated general illness. Pain and limp is intermittent initially and becomes gradually more persistent. Mobility of the hip joint is reduced if there is already some deformity of the femoral head, the affected leg is slightly shortened.
DIAGNOSIS
The condition is diagnosed by X-rays in the established cases or by bone scan in the early cases. Other investigations include MRI (magnetic resonant imaging ) and ultrasonography. Perthes' disease can elude diagnosis in the early stages and may be confused with other conditions that also cause hip pain e.g. Transient synovitis, Rheumatoid arthritis, Septic arthritis.
TREATMENT
The aims of treatment are to reduce hip irritability and stiffness, prevent deformity of the femoral head and protect the hip through the period of healing. More than 50% of children affected by Perthes' disease do very well without any active treatment. These are the children who acquire the disease when they are 5 years or younger, and those in whom only a small portion of the femoral head is affected. These children require only regular check ups and occasional confinement to bed to treat hip pain and stiffness. Most doctors will advise against impact sports e.g. jumping and running on hard surfaces for a period of two years.
Children who acquire the condition after 8 years of age may not benefit from active treatment. These children tend to develop more hip deformity and have less good outcome. They will nonetheless have hips that will function quite well for many years. There is a higher probability of hip arthritis after the age of 45 years.
Children with the condition between the ages of 5 to 8 years require careful evaluation to decide if they require treatment. Opinions amongst medical practitioners differ widely and there is as yet no generally agreed protocol for treatment. Although all doctors agree that it is desirable to prevent hip deformity we cannot agree on how best to achieve this aim or even whether we can influence the development of hip deformity.
The majority of doctors involved in the care of children's orthopaedics believe that femoral head deformity can be minimised or prevented by keeping the head under the protective cover of the acetabulum ( Principles of Containment), provided treatment is carried out at an appropriate early stage of the disease. Containment can be by means of an abduction brace in which the head is kept under protective cover of the acetabulum by restricting motion within a selected range, or by surgically redirecting the femoral head ( Femoral Osteotomy ) or acetabulum ( Innominate Osteotomy ) to provide the cover.
The difference in results of operative and non-operative treatment has not been conclusively determined. There are advantages and disadvantages with both methods of treatment. The duration of treatment by bracing varies with the age of the child and to some extent the degree of head involvement. Braces are usually required for at least 2 years. If treatment by brace is selected, compliance to treatment is essential. If a child will not comply to brace treatment, operative treatment may be more appropriate.
An operation eliminates the need for constant supervision of the child, but one should be reminded that this option involves a significant and skilled surgical undertaking under general anaesthesia. The choice of operative technique is beyond the scope of this article but you are advised that the operation does not hasten the healing of the condition. A femoral osteotomy may cause slight shortening of the leg. An innominate osteotomy lengthens the leg slightly. It is unusual for either forms of operations to require blood transfusion.
Recovery from an operation involves variably 1 to 3 weeks of hospitalization and use of crutches for about 6 weeks.Some surgeons employ a plaster hip spica to protect an innominate osteotomy. In both forms of operations metallic implants are necessary for fixation of the osteotomies. These metal implants are usually removed under general anaesthesia some weeks or months later.
 Dr. Leonard kuo
Dr. Leonard kuo